|
Precious-Information - To know Your BodyTimely - Awareness - Can Save - Salvage Precious Body FunctionsPrecious-Information here is part of contribution to improve general awareness of some Medical & Surgical Emergencies, I have been requested to add some key Medical & Surgical Emergencies. Accordingly I will be adding few. Most important - always please seek Competant expert advise, Don't ignore the Symptom. Identify - Recognise Treat the Cause - Not just the Symptom - Your Health Matters For You, Us & Others. Look after Your Body. As you know "A stich in Time Saves nine". Surgical Emergency 1:Testicular Torsion [Twisted Testes Syndrome Or Torsion of the Spermatic Cord ] Custom Search
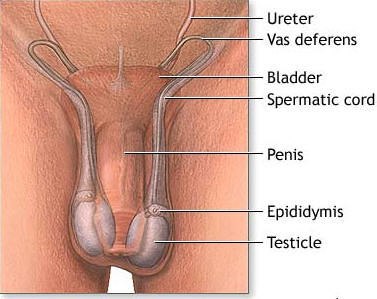
The Basic Anatomy:
The Intra-Operative finding:
Introduction/Background: Torsion of the testis, or more correctly, torsion of the spermatic cord, is a surgical emergency because it causes strangulation of gonadal blood supply with subsequent testicular necrosis and atrophy. Acute scrotal swelling in children indicates torsion of the testis until proven otherwise. In approximately two thirds of patients, history and physical examination are sufficient to make an accurate diagnosis. History of the Procedure Patients often complain of acute-onset scrotal discomfort, which may occur at rest or may relate to sports or physical activities. They may describe similar previous episodes, which may suggest intermittent testicular torsion. 1 Patients deny voiding problems or painful urination but may describe nausea and vomiting.ProblemTesticular torsion refers to twisting of the spermatic cord structures, either in the inguinal canal or just below the inguinal canal. The following are the 2 most common types of testicular torsion are as above (see images). Testicular torsion is a true urologic emergency and must be differentiated from other complaints of testicular pain because a delay in diagnosis and management can lead to loss of the testicle. Though testicular torsion can occur at any age, including the prenatal and perinatal periods, it most commonly occurs in adolescent males; it is the most frequent cause of testicle loss in that population. The testicle is covered by the tunica vaginalis, a potential space that encompasses the anterior two thirds of the testicle and where fluid from a variety of sources may accumulate. The tunica vaginalis attaches to the posterolateral surface of the testicle and allows for little mobility of the testicle within the scrotum. In patients who have an inappropriately high attachment of the tunica vaginalis, the testicle can rotate freely on the spermatic cord within the tunica vaginalis (intravaginal testicular torsion). This congenital anomaly, called the bell clapper deformity, can result in the long axis of the testicle being oriented transversely rather than cephalocaudal. This congenital abnormality is present in approximately 12% of males, 40% of whom have the abnormality in the contralateral testicle as well. The bell clapper deformity allows the testicle to twist spontaneously on the spermatic cord. Torsion occurs as the testicle rotates between 90° to 180°, causing compromised blood flow to the testicle. Complete torsion usually occurs when the testicle twists 360° or more; incomplete or partial torsion occurs when the twisting is less than this. The twisting of the testicle causes venous occlusion and engorgement as well as arterial ischemia and infarction of the testicle. How tightly the testicle is twisted appears to correlate with how quickly the testicle becomes nonviable from ischemia. In the neonatal age group, the testicle frequently has not yet descended into the scrotum, where it becomes attached within the tunica vaginalis. This mobility of the testicle predisposes it to torsion (extravaginal testicular torsion). Inadequate fusion of the testicle to the scrotal wall typically occurs within the first 7-10 days of life. Frequency: Incidence of torsion in males younger than 25 years is approximately 1 in 4000. Torsion more often involves the left testicle. Of the cases of testicular torsion that occur in the neonatal population, 70% occur prenatally and 30% occur postnatally.Mortality/Morbidity This urologic emergency requires prompt diagnosis, immediate urologic consultation, and rapid definitive operative treatment for salvage of the testicle. A salvage rate of 90-100% is found in patients who undergo detorsion within 6 hours of pain; the viability rate fell to between 20% and 50% after 12 hours; and 0 to 10% viability if detorsion is delayed greater than 24 hours. AgeTesticular torsion most often is observed in males younger than 30 years, with most aged 12-18 years. The peak age is 14 years, although a smaller peak also occurs during the first year of life. Clinical History: • History includes a sudden onset of severe unilateral scrotal pain. • Onset of pain can occur more slowly, but this is an uncommon presentation of torsion. • Torsion can occur with activity, can be related to trauma in 4-8% of cases,2 or can develop during sleep. • The historical features suggestive of testicular torsion include the following: o Acute onset of unilateral scrotal pain o Scrotal swelling o Nausea and vomiting: In the pediatric population, nausea and vomiting more commonly accompany acute testicular torsion and have a positive predictive value of greater than 96%. o Abdominal pain (20-30%) o Fever (16%) o Urinary frequency (4%) • Many patients have a history of recurrent scrotal pain that has resolved spontaneously. This history is highly suggestive of intermittent torsion and detorsion of the testicle. Patients who complain of what sounds like torsion-detorsion should be referred promptly to a urologist since patients with symptoms of intermittent torsion who electively have surgical exploration are less likely to develop subsequent torsion and loss of the testicle. Creagh et al reported that acute torsion developed in 10% of patients with intermittent torsion while they waited for surgery. Treatment Emergency Department Care: • Early diagnosis and prompt urologic consultation is essential since time is critical in salvage of the testicle. • Analgesic pain relief should be administered as testicular torsion is typically very painful. • Attempt manual detorsion with pain relief as the guide for successful detorsion. The procedure is similar to the "opening of a book" when the physician is standing at the patient's feet. • Most torsions twist inward and toward the midline; thus, manual detorsion of the testicle involves twisting outward and laterally. o For example, in a suspected torsion of the right testicle, the physician is in front of the standing or supine patient and holds the patient's right testicle with the left thumb and forefinger. o The physician then rotates the right testicle outward 180° in a medial to lateral direction. o Rotation of the testicle may need to be repeated 2-3 times for complete detorsion and to provide pain relief to the patient. o For the patient's left testicle, the physician uses the right thumb and forefinger and rotates the patient's left testicle in an outward direction 180° from medial to lateral. o Manual detorsion is successful in 26.5% to greater than 80% of patients based upon a number of reviewed studies. Consultations If the clinical diagnosis of torsion is suspected, early urologic consultation is mandatory since definitive treatment is surgery for detorsion and orchiopexy or possible orchiectomy. Treatment Medical Therapy Manual detorsion of the torsed testis may be attempted but is usually difficult because of acute pain during manipulation. This nonoperative detorsion is not a substitute for surgical exploration. If successful (ie, confirmed by color Doppler sonogram in a patient with complete resolution of symptoms), perform definitive surgical fixation of the testes before the patient leaves the hospital as an urgent—rather than emergent—procedure. Surgical Therapy Treatment of testicular torsion varies according to patient age. • Treat patients who are born with testicular torsion by performing early elective exploration and contralateral orchidopexy (anchoring) because bilateral (synchronous or asynchronous) neonatal testicular torsion is described. • The potential for salvage of such a testis is nil, making the risk of immediate surgery before complete stabilization of the newborn unwarranted. • In distinct contrast, a newborn with a normal testis at birth who subsequently undergoes torsion requires immediate exploration. • Perform the operation through the midline scrotal raphe. • Enter the ipsilateral scrotal compartment; then, deliver and untwist the testis. • Evaluate the testis for viability. • Remove the necrotic testis to avoid prolonged, debilitating pain and tenderness. Retention of a necrotic testis may exacerbate the potential for subfertility, presumably because of development of an autoimmune phenomenon. • To prevent subsequent torsion, fix viable gonads to the scrotal wall with 3-4 nonabsorbable sutures. Perform both exploration and anchoring of the contralateral testis through the same incision.Intraoperative DetailsSigns of a viable testis after detorsion (see image below) include a return of color, return of Doppler flow, and arterial bleeding after incision of tunica albuginea. MedicationAnalgesic pain relief should be administered for testicular torsion.AnalgesicsPain control is essential to quality patient care. It ensures patient comfort, promotes pulmonary toilet, and enables physical therapy regimens. Most analgesics have sedating properties, which are beneficial for patients who have sustained painful trauma. Follow-up Transfer • Transfer the patient if no urologist is available.Complications Complications of testicular torsion may include the following:• Infarction of testicle • Loss of testicle • Infection • Infertility secondary to loss of testicle • Cosmetic deformity Prognosis • If testicular torsion is diagnosed early, a near 100% salvage rate for the testicle is possible. Orchiopexy is not a guarantee against future torsion, though it does reduce the odds of a future torsion. Patient Education • For excellent patient education resources, visit eMedicine's Men's Health Center. Also, see eMedicine's patient education article Testicular Pain. MiscellaneousMedicolegal Pitfalls • Failure to recognize a urologic emergency • Delay in obtaining urologic consultation • Misdiagnosing as epididymitis • Incomplete reduction of a torsion Credits: My gratitude, Thanks, Appreciations to: My Urology & friends, associates – world-wide, incl:International Surgical Charity Associates [ISCA], Dr Timothy J Rupp, MD, FACEP, Associate Medical Director, Physicians Emergency Care Associates, Methodist Health System, Dallas, Texas; Staff Physician, Innovative Emergency Medicine, Frisco, Texas; Staff Physician, Department of Emergency Medicine, Children's Medical Center of Dallas, Dallas, TexasDr Mark Zwanger, MD, MBA, Assistant Professor, Department of Emergency Medicine, Thomas Jefferson University Dr Eugene Minevich, MD, Assistant Professor, Department of Surgery, Division of Pediatric Urology, University of Cincinnati Dr Leslie Tackett McQuiston, MD, FAAP, Assistant Professor of Surgery (Urology) Dartmouth Medical School; Staff Pediatric Urologist, Dartmouth-Hitchcock Hospital All those who requested to add some key Medical & Surgical Emergencies. Disclaimer: This is mainly to improve basic general awareness for some important emergency conditions. Please seek expert competant Medical &/Or Surgical advise for prompt appropriate management. We will be adding few more as per further requests. Dr Raj Vastrad & International Surgical Charity Associates [ISCA] Custom Search
|